



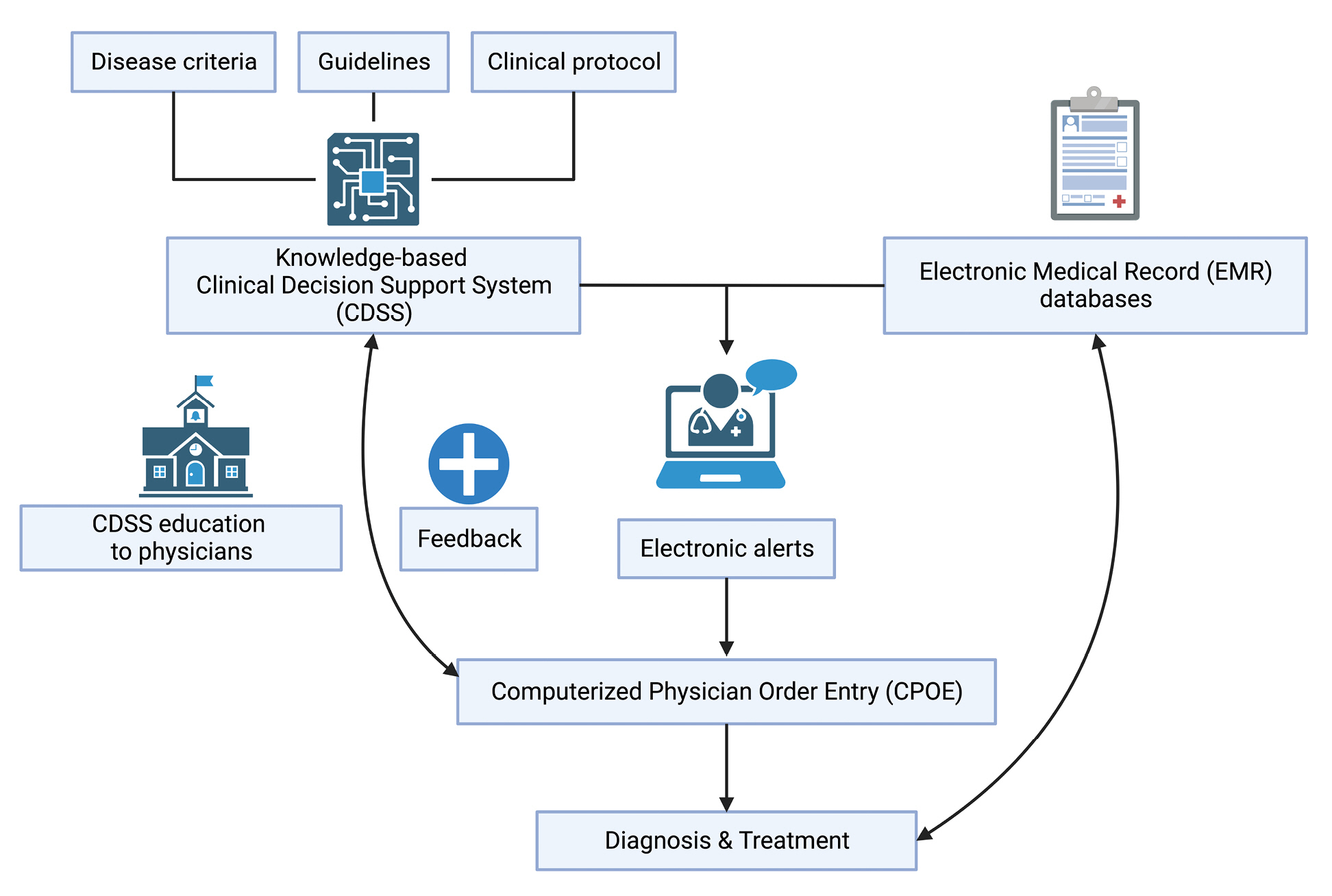
Clinical decision support systems (CDSS) are computer-based programs designed to improve patient care by providing patient-specific information and clinical knowledge to healthcare professionals [1]. These systems were developed to improve clinical decision-making by integrating relevant data and offering tailored recommendations based on individual patient characteristics. CDSS are already widely used in hospital settings in forms of alerting physicians and other healthcare professionals regarding medication interactions, potential diagnoses, and treatment alternatives. These systems can aid healthcare professionals in enhancing patient safety and improving clinical outcomes by offering timely and relevant data to minimize medical errors. A randomized trial demonstrated the effectiveness of electronic alert systems in reducing drug interactions [2]. CDSS can also assist with disease management, clinical protocols, and guideline adherence. For example, the system for an asthma attack, entitled ‘ACAFE (Asthma Clinical Assessment Form and Electronic) decision support’, improved asthma plan provision, documentation of asthma severity, and other important clinical parameters [3].
Park et al. [4] performed a retrospective cohort study to demonstrate the impact of CDSS in patients at risk of acute kidney injury (AKI) after contrast-enhanced computed tomography (CECT). They compared two time periods (before and after) according to the initiation of a new electronic alert system as CDSS. The alert system was activated when CECT was prescribed for patients undergoing kidney replacement therapy or with a baseline estimated glomerular filtration rate (eGFR) of < 45 mL/min/1.73m2. Although the incidence and major outcomes of AKI were similar between the two groups, the frequency of kidney function monitoring by nephrologists significantly increased from 29.4% to 66.7% and the volume of prophylactic fluid was smaller in the alert group compared to the historical control group.
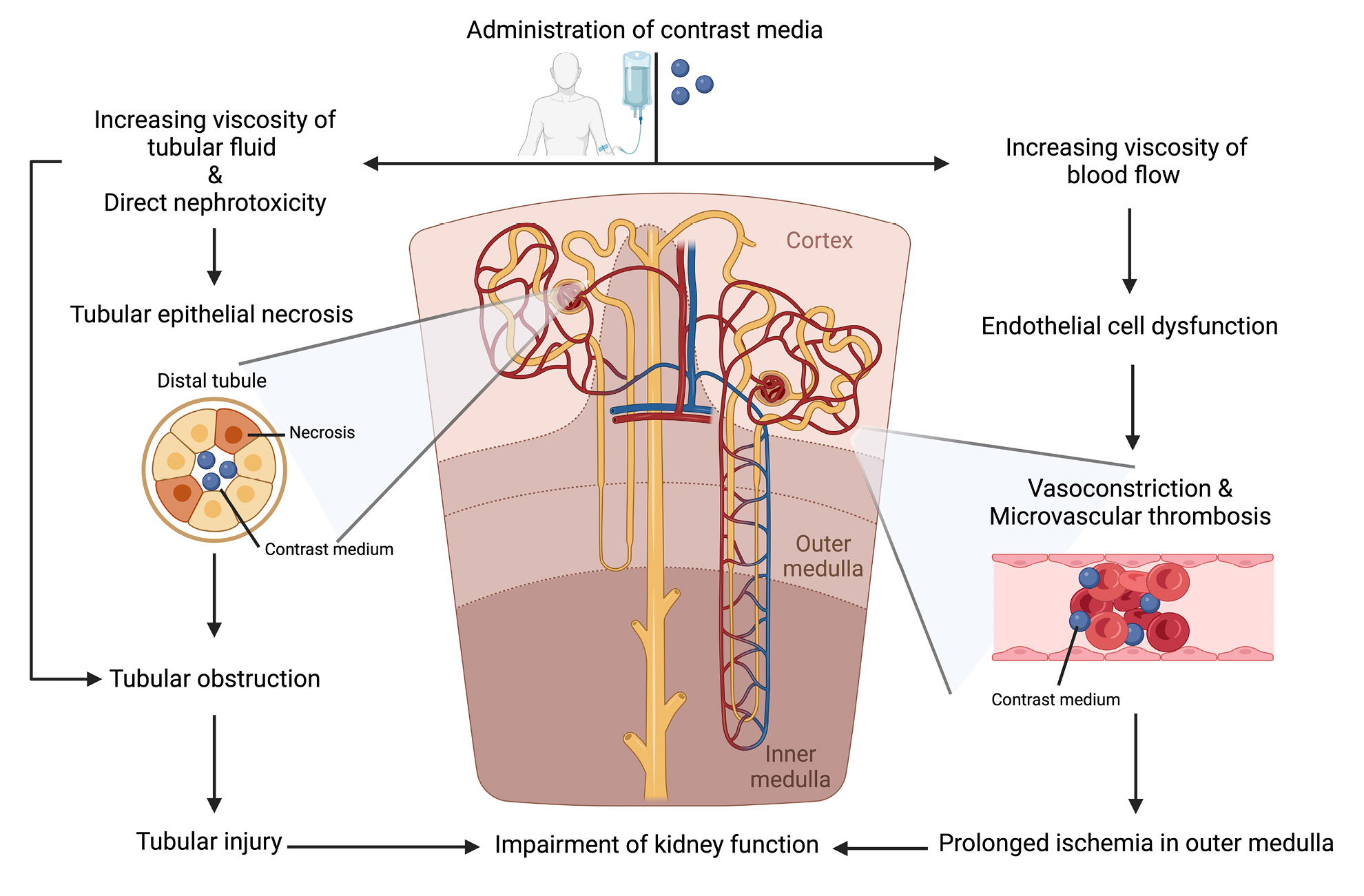
Extensive use of intravenous contrast media for CECT or radiologic interventions has been associated with an increased risk of AKI. The Contrast Media Safety Committee (CMSC) of the European Society of Urogenital Radiology (ESUR) defined ‘post-contrast acute kidney injury (PCAKI)’ as a sudden deterioration in kidney function within 48 hours after intravascular administration of iodine-based contrast media [5]. The pathogenesis of PCAKI involves two distinct pathways: direct nephrotoxic effects of contrast media and indirect disturbances in kidney blood flow (Fig. 1) [6]. Direct effects are caused by contrast media-induced adverse changes in tubular flow and physiology, including increased viscosity, loss of polarity in tubular cells, and the subsequent apoptosis and necrosis in tubular cells, leading to tubular obstruction and injury. Indirect effects arise from elevated blood viscosity, which disrupts normal blood flow patterns and causes endothelial dysfunction [7,8]. These effects are accompanied by increased endothelin levels, activation of the renin-angiotensin system, and reduced levels of nitric oxide and prostaglandin I2, resulting in vasoconstriction of renal arterioles. These indirect effects can further lead to microvascular thrombosis and prolonged ischemia in the renal medulla. Ultimately, the overall harmful effects caused by contrast media deteriorate kidney function. In a multicenter cohort study including 288 hospitalized patients diagnosed with PCAKI, the incidence of persistent kidney dysfunction was 46.9% and the all-cause mortality rate for 1 year was as high as 13.5% [9]. The risk factors of PCAKI included age, preexisting kidney dysfunction, proteinuria, hypertension, and diabetes mellitus [10,11]. CMSC recommended eGFR measurements within 7 days before contrast media exposure for patients with acute illness or acute deterioration of preexisting chronic disease and for inpatients [11]. PCAKI following CECT is associated with all-cause mortality and subsequent chronic kidney disease (CKD) after severe or persistent PCAKI may impede the optimal evaluation and treatment of primary illnesses [12]. Therefore, systemized strategies for early detection and prevention of PCAKI are critical for avoiding unfavorable clinical outcomes and progression of CKD especially in patients receiving repeated CECT due to underlying diseases such as cancer. Since intravenous fluid therapy, specifically intravascular volume expansion, has been reported as a preventive measure for PCAKI, the ESUR recommended preventive fluid therapy to reduce the risk of PCAKI in all patients with risk factors [11,13,14]. The recommended intravenous fluid regimens for preventing PCAKI include the administration of either 3 mL/kg/hr of bicarbonate 1.4% (or 154 mmoL/L solution) for 1 hour before contrast media (in the case of intra-arterial administration, followed by 1mL/kg/hr of bicarbonate 1.4% for 4 to 6 hours after contrast media) or 1 mL/kg/hr of 0.9% saline for 3 to 4 hours before and 4 to 6 hours after contrast media infusion [11].
It is noteworthy that Park et al.’s study [4] did not find a significant difference in the incidence of PCAKI despite of fluid volume difference between the groups. The volume of administered fluid in the alert group (750 mL of isotonic fluid) was lower than that in the control group (1,000 mL of isotonic fluid). Administering large volume of fluids can cause intrarenal venous congestion and compartment syndrome because kidneys are encapsulated organs [15]. Thus, careful monitoring of volume status and administration of the optimal volume of prophylactic fluid are imperative to prevent PCAKI. In an outpatient clinic-based management for PCAKI, the shortening of fluid infusion time is preferred. Reduction of fluid volume by the alert system in Park’s study [4] may contribute to the establishment of an optimized fluid protocol for patients undergoing CECT in outpatient clinics.
Although there were no statistically significant differences in the incidence of PCAKI, the risk of hospitalization, and kidney replacement therapy following the implementation of an electronic alerts system, the frequency of consultation and follow-ups with nephrologists were increased by the alert system in Park’s study [4]. There were several studies to determine the efficacy of CDSS for AKI. In a randomized study with 1,201 patients assigned to the AKI alert group and 1,192 patients assigned to the control group, the primary outcomes including relative maximum changes in serum creatinine, dialysis, and mortality within 7 days were comparable between the groups [16]. Despite insufficient data demonstrating the effectiveness of an AKI alert system on overall kidney outcome and mortality, early detection of AKI and timely consultation with nephrologists by an alert system are anticipated to contribute to the earlier management of AKI and the improvement of patient overall outcomes including mortality [17]. The effectiveness of CDSS in reducing the occurrence of overlooked AKI cases was reported by showing that early nephrology consultation was linked to improved clinical outcomes in hospitalized patients [18]. Consequently, the implementation of an electronic AKI alert system holds promising potential to improve patient outcomes.
In a previous study with AKI patients, alerts without CDSS education were associated with a significantly increased risk of mortality [19]. In a randomized controlled study [20], the efficacy of an intervention comprising of education on AKI, PCAKI prevention approaches, safe target volumes of contrast, and feedback was investigated for the prevention of AKI following coronary angiography or percutaneous coronary intervention. In this study, the intervention groups showed a lower likelihood of developing PCAKI compared to the control group, supporting the importance of comprehensive CDSS education to physicians and implementation of adequate management strategies for AKI. The presence of well-educated physicians who are proficient in CDSS utilization holds the potential to improve the prognosis of PCAKI and overall patient outcomes.
In Park et al.'s study [4], the electronic alert system for outpatient protocol based on CDSS effectively reduced the volume of preventive fluid therapy without an increase in the incidence of PCAKI and facilitated active consultations with nephrologists after CECT. Therefore, CDSS-based electronic alert system seem to have the potential to prevent PCAKI or mitigate the severity of AKI in patients with risk factors. To advance the effectiveness of CDSS for PCAKI prevention, education on PCAKI and the implementation of an electronic alert system are critically required (Fig. 2). Although there is some evidence supporting the efficacy of CDSS in improving patient care, further prospective studies are required to refine the design of these systems and enhance the optimal utilization of a CDSS-based electronic alert system in clinical practice.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









